Additional information from Singapore, comparing viral loads over time among both vaccinated and unvaccinated people. It confirms that in the beginning, viral loads are indeed similar, but over time, the vaccinated people eliminate their viral loads at a much faster pace, which would explain the high protective effect against hospitalization and death. (not yet peer reviewed)
Objectives Highly effective vaccines against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) have been developed but variants of concerns (VOCs) with mutations in the spike protein are worrisome, especially B.1.617.2 (Delta) which has rapidly spread across the world. We aim to study...

www.medrxiv.org
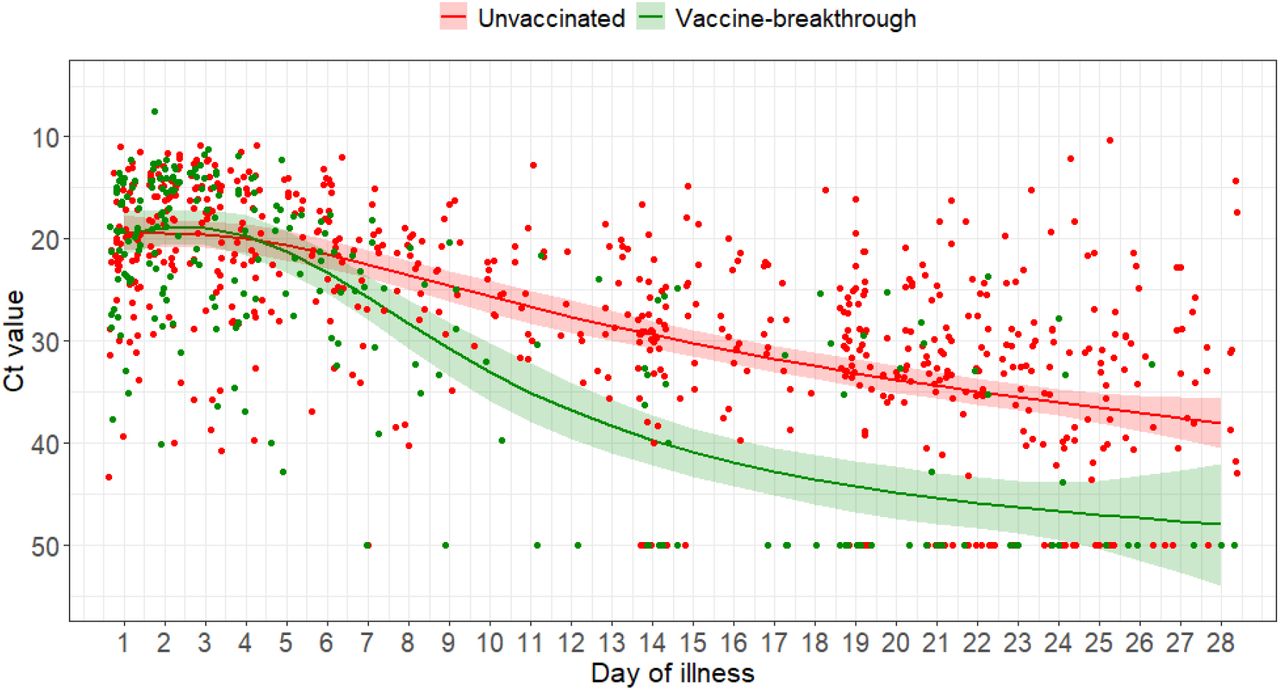
Serial Ct values of individuals were analyzed as a surrogate marker for the viral load. The initial median initial Ct value did not differ between unvaccinated and fully vaccinated patients (unvaccinated median Ct 18.8 (14.9-22.7), vaccinated 19.2 (15.2-22.2), p=0.929). However, fully vaccinated patients had a faster rate of increase in Ct value over time compared with unvaccinated individuals, suggesting faster viral load decline (coefficient estimates for interaction terms ranged from 9.12 (standard error 3.75) to 12.06 (standard error 3.03); p-value <0.05 for each interaction terms) (
Figure 1).
In this study, we found that fully vaccinated patients had significantly lower odds of moderate or severe outcomes following infection by the SARS-CoV-2 VOC B.1.617.2. Vaccination was associated with lower peak measures of systemic inflammation, fewer symptoms, including more asymptomatic infection, and better clinical outcomes. Notably, in contrast to existing studies that showed lower viral load in vaccinated patients [
22], initial viral load indicated by PCR Ct values was similar between vaccinated and unvaccinated patients with B.1.617.2. However, vaccinated patients appeared to clear viral load at a faster rate. Our serologic data suggest an early rapid rise in neutralizing and binding antibodies indicated by C-Pass and Roche anti-S antibodies, which may be evidence of memory immunity to COVID-19 vaccination on challenge with a breakthrough infection with B.1.617.2.
The finding of diminished severity with B.1.617.2 infection in vaccinated individuals is reassuring and corroborates emerging data from the United Kingdom which have found that mRNA vaccination remains protective against symptomatic and severe disease[
12,
23]. An observational cohort study conducted in Scotland suggested that ≥14 days after the second dose, BNT162b2 vaccine offered 92% vaccine effectiveness against presumptive non-B.1.617.2 infection and 79% protection against presumptive B.1.617.2 [
24]. Protection associated with the ChAdOx1 nCoV-19 vaccine was 73% and 60% respectively. Although vaccine-breakthrough infections are increasingly reported, with the largest series to date in the United States reporting 10,262 breakthrough infections, a majority of these were mild (27% asymptomatic, 10% hospitalization, 2% mortality)[
25]. Vaccine-breakthrough infections will continue to be observed, especially with genetic drift and selection pressures resulting in emergence of newer VOCs; however, it is likely that there will be a shift toward milder disease spectrum with more widespread implementation of vaccination programs.
mRNA vaccines against COVID-19 are protective against symptomatic infection and severe disease by the B.1.617.2 variant. Vaccinated individuals had a more rapid decline in viral load, which has implications on secondary transmission and public health policy. Rapid and widespread implementation of vaccination programs remains a key strategy for control of COVID-19 pandemic. Further studies should elucidate immunologic features driving vaccine-breakthrough infection to improve vaccine-induced protection.